The hip is a ball and socket joint. The joint is involved in simply daily activities such as getting in and out of bed or the car, getting dressed, walking and climbing stairs. Moreover, the hip is involved with dynamic movements such as running, soccer, and other sporting events. In this article, we will review the anatomy and functional anatomy of the hip, biomechanics of hip movement, what hip osteoarthritis (O.A.) is, the types of total hip surgical procedures and the evidenced based training approach, to work with either a client who has O.A. or underwent a THR.
The hip joint is covered by a capsule blended with three strong ligaments: iliofemoral or Y ligament, which resists extension, the ischiofemoral ligament, which resists extension and internal rotation, and the pubofemoral ligament, which resists abduction. Additionally, the acetabular labrum, is a ring of cartilage that surrounds the acetabulum. The function of the labrum is to provide stability so that the femoral head doesn't sublux or slip out of the acetabulum.
Glute medius originates on surface of the iliac crest, it inserts to the lateral surface of the greater trochanter. Whereas, the glute minimus originates along outer surface of the ilium between the anterior & inferior gluteal lines of sciatic notch and inserts along anterior aspect of the greater trochanter. Both glute medius and minimus abduct and internally rotate the hip. Glute maximus is the 'powerhouse,' which extends and laterally rotates the hip.
The research shows that both the glute medius and minimus are weaker in women and more prone to developing patellofemoral syndrome (Lankhorst et al 2012 & Khayambashi, H., et al. 2012 & Meira et al. 2011).
During hip extension, the femoral head translates back and up as the glute maximus creates a backward (concentrically contracts) tensioning the iliofemoral ligaments, hip flexors eccentrically contracts.
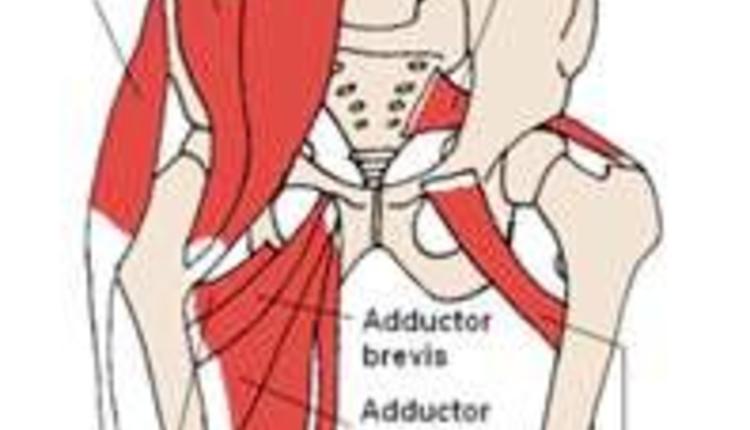
During hip abduction, the femur outwardly translates and the movement is restrained by the adductors (adductor magnus and brevis primarily) as the pubiofemoral ligament is tensioned.
a. Negotiating stairs - in order to climb stairs, there has to be adequate ankle mobility to plantar flex the foot,
bend the knee and flex the hip to clear the stair.
b. Getting dressed in the morning - a simple activity that everyone does every day is getting dressed and either putting on slacks or pants. This requires hip flexion, external rotation and abduction of the hips, followed by hip adduction.
a. Hip osteoarthritis (O.A.)
Pathophysiology: Is a degenerative process of varied etiology, which includes mechanical changes that occur within the joint. O.A. (Pisters, M., et al 2007). Osteoarthritis is the most common form of arthritic disorders and is one of the most common reasons for visiting a health professional. The hip is a common site for O.A., affecting between 25-40% of population over 55 years of age (Sutlive, T. 2008 & Zhang, W., et al. 2007).
Risk Factors: Excessive weight born on hip joint, muscle imbalance and repetitive stressors.
Sign and symptoms: Pain in the morning is described as achy, where patients experience pain particularly with weight bearing activities such as walking and have difficulty squatting. Patients will describe of pain and stiffness in the morning described as achy. During the day, with both movement and activity, improves mobility and activity (Fernandes, L et al 2010). However, if the volume of activity is too much, pain will increase.
Objective findings: Individuals with hip O.A. will present with gross limitation or a capsular pattern, where hip internal rotation is most limited, followed by hip flexion and abduction (Sutlive 2008). In addition, those with hip O.A. will complain of morning stiffness, and demonstrate decreased hip mobility, whereby hip internal rotation is less than 15 degrees.
Medical management: Radiographs represent the current gold standard for diagnosing O.A. Non steroidal (NSAIDS) (examples are Ibuprofen/Advil).
Recommendations for training clients with hip O.A.: Aqua therapy has been shown in the research to significantly reduce pain, improved physical function and mobility, strength and quality of life(Hinman, Rana S., et al 2007). It is important to stretch the tight iliotibial band, hip flexors, quadriceps and hamstrings to improve mobility. Then strengthen phasic (weaker) hip abductors (glute medius and minimus).
Strengthening specifically hip abductors in various studies, when compared to general strengthening resulted in significant reduction in knee pain, objective change in functional outcome tests, physical function and daily activities(Bennell,K.L., et al. 2010 & Hernández-Molina, G. et al. 2008). Core strengthening should also be an integral part of the training program and personalized.
Exercises to avoid: Single leg and deep squats (places excessive compression forces on hip joint).
The determination to undergo a total hip replacement is primarily based and decided by both the surgeon and patient. Whereby a patient has significant inability to perform daily functional activities, experiences severe pain and lacks functional mobility.
Hip replacement (THR)
In traditional hip replacement surgery, the surgeon makes a long incision and cuts various muscles, tendons and ligaments to get to the hip joint. When more tissues, muscles and tendons are cut during surgery, the recovery is more painful and the healing process takes longer.
Hip replacement surgery has evolved into one of the most frequently performed reconstructive procedures today. In the total hip replacement surgery, the surgeon can perform either a posterior (back), lateral or anterior (front) approach.
Recommendations for training: Important to follow hip precautions: avoidance of crossing affected leg towards midline (adduction) and squatting past hip flexion 90 degrees.
Training should focus on strengthening weak glute medius and minimus, glute maximus and hamstring muscles.
Effective and safe exercises include: in place lunges, diagonal lunges, seated leg extension and seated leg curl machine.
Core strengthening should also always begin with static exercises and then progressed to dynamic accordingly. Safe and effective core strengthening exercises include standing trunk rotation with tubing or cable, four-point planks and side planks. Safe dynamic core strengthening exercises include bridging with physioball, single leg bridge with physioball, traveling forward lunge with medicine ball trunk rotation and four-point plank on physioball as examples.
Contraindications to training: Patient should avoid deep squatting and single leg squats, which can compromise the prosthesis, making it susceptible for dislocation and creating deep hip pain.
The hip is a complex unit that is comprised of a multitude of ligaments, tendons, connective tissue and muscles that synergistically initiate and correct movement and stabilize in an unstable environment. Understanding the anatomy, biomechanics and weak links of the hip, common injuries and evidenced-based training strategies, should provide you with the insight to better understand and work with clients with these kind of injuries more confidently.
REFERENCES
Bennell, K.L., et al., 2010, 'Hip strengthening reduces symptoms but not knee load in people with medial knee osteoarthritis and varus malalignment: a randomized controlled trial,' Journal of Osteoarthritis and Cartilage, vol. 18, issue 5, pp. 621-628.
Cyriax, J. 1982, Textbook of Orthopedic Medicine, Volume 1: Diagnosis of Soft Tissue Lesions. London, UK. Baillere Tindall.
Fernandes, L., et al 2010, 'Efficacy of patient education and supervised exercise vs. patient education alone in patients with hip osteoarthritis: a single blind randomized clinical trial,' Osteoarthritis and Cartilage, vol. 18, issue 10, pp. 1237–1243.
Hernández-Molina, G., et al., 2008, 'Effect of therapeutic exercise for hip osteoarthritis pain: Results of a meta-analysis,' Journal of Arthritis Care & Research, vol. 59, issue 9, pp. 1221–1228.
Hinman, Rana S., et al 2007, 'Aquatic Physical Therapy for Hip and Knee Osteoarthritis: Results of a Single-Blind Randomized Controlled Trial,' Journal of Physical Therapy, vol. 87, no. 1, pp. 32-43.
Khayambashi, H., et al., 2012, 'The Effects of Isolated Hip Abductor and External Rotator Muscle Strengthening on Pain, Health Status, and Hip Strength in Females With Patellofemoral Pain: A Randomized Controlled Trial,' Journal of Orthopedic Physical Therapy, vol. 42, no. 1, pp. 22-29.
Lankhorst, N, et al, 2012, 'Risk Factors for Patellofemoral Syndrome: A Systematic Review,' JOSPT, vol. 42, No. 2, pp. 81-90.
Meira, E., et al., 2011, 'Influence of the Hip on Patients With Patellofemoral Pain Syndrome,' Sports Health, vol. 3, issue 5, pp. 455–465.
Pisters, M., et al., 2007, 'Exercise adherence improving long-term patient outcome in patients with osteoarthritis of the hip and/or knee,' Arthritis Care & Research, vol. 62, issue 8, pp. 1087-1094.
Prock, S., 2007, 'Initial results with a mini-posterior approach for total hip arthroplasty,' International Orthopedics, vol. 31, supplemental 1, pp. 17–20.
Sutlive, T., et al, 2008, 'Development of a Clinical Prediction Rule for Diagnosing Hip Osteoarthritis in Individuals With Unilateral Hip Pain,' JOSPT, vol. 38, no. 9, pp. 542-548.
Zhang, W., et al., 2007, 'OARSI recommendations for the management of hip and knee osteoarthritis, Part I: Critical appraisal of existing treatment guidelines and systematic review of current research evidence,' Osteoarthritis and Cartilage, vol. 15, issue 9 pp. 981–1000.
Basic anatomy
Let's look at the basic anatomy of the hip. The hip joint is a multi-axial ball and socket joint between the femoral head and the acetabulum, similarly to the shoulder joint. There are several ligaments that surround the hip providing both support and stability.The hip joint is covered by a capsule blended with three strong ligaments: iliofemoral or Y ligament, which resists extension, the ischiofemoral ligament, which resists extension and internal rotation, and the pubofemoral ligament, which resists abduction. Additionally, the acetabular labrum, is a ring of cartilage that surrounds the acetabulum. The function of the labrum is to provide stability so that the femoral head doesn't sublux or slip out of the acetabulum.
Hip musculature
Muscularly, there are several dynamic hip stabilizing muscles. The primary stabilizing muscles include the glute medius, glute minimus and glute maximus muscles.Glute medius originates on surface of the iliac crest, it inserts to the lateral surface of the greater trochanter. Whereas, the glute minimus originates along outer surface of the ilium between the anterior & inferior gluteal lines of sciatic notch and inserts along anterior aspect of the greater trochanter. Both glute medius and minimus abduct and internally rotate the hip. Glute maximus is the 'powerhouse,' which extends and laterally rotates the hip.
The research shows that both the glute medius and minimus are weaker in women and more prone to developing patellofemoral syndrome (Lankhorst et al 2012 & Khayambashi, H., et al. 2012 & Meira et al. 2011).
Hip Biomechanics
During hip flexion, the femoral head translates up and down (inferior) as the glute maximus eccentrically pulls and tensions the iliofemoral, pubofemoral and ischiofemoral ligaments.During hip extension, the femoral head translates back and up as the glute maximus creates a backward (concentrically contracts) tensioning the iliofemoral ligaments, hip flexors eccentrically contracts.
During hip abduction, the femur outwardly translates and the movement is restrained by the adductors (adductor magnus and brevis primarily) as the pubiofemoral ligament is tensioned.
Functional Anatomy
When we look at daily activities that involve the hip, there are several. Let’s look at two common functional tasks that everyone performs on a daily basis. The first is climbing stairs.a. Negotiating stairs - in order to climb stairs, there has to be adequate ankle mobility to plantar flex the foot,
bend the knee and flex the hip to clear the stair.
b. Getting dressed in the morning - a simple activity that everyone does every day is getting dressed and either putting on slacks or pants. This requires hip flexion, external rotation and abduction of the hips, followed by hip adduction.
What is Hip Osteoarthritis (O.A.)?
a. Hip osteoarthritis (O.A.)
Pathophysiology: Is a degenerative process of varied etiology, which includes mechanical changes that occur within the joint. O.A. (Pisters, M., et al 2007). Osteoarthritis is the most common form of arthritic disorders and is one of the most common reasons for visiting a health professional. The hip is a common site for O.A., affecting between 25-40% of population over 55 years of age (Sutlive, T. 2008 & Zhang, W., et al. 2007).
Risk Factors: Excessive weight born on hip joint, muscle imbalance and repetitive stressors.
Sign and symptoms: Pain in the morning is described as achy, where patients experience pain particularly with weight bearing activities such as walking and have difficulty squatting. Patients will describe of pain and stiffness in the morning described as achy. During the day, with both movement and activity, improves mobility and activity (Fernandes, L et al 2010). However, if the volume of activity is too much, pain will increase.
Objective findings: Individuals with hip O.A. will present with gross limitation or a capsular pattern, where hip internal rotation is most limited, followed by hip flexion and abduction (Sutlive 2008). In addition, those with hip O.A. will complain of morning stiffness, and demonstrate decreased hip mobility, whereby hip internal rotation is less than 15 degrees.
Medical management: Radiographs represent the current gold standard for diagnosing O.A. Non steroidal (NSAIDS) (examples are Ibuprofen/Advil).
Recommendations for training clients with hip O.A.: Aqua therapy has been shown in the research to significantly reduce pain, improved physical function and mobility, strength and quality of life(Hinman, Rana S., et al 2007). It is important to stretch the tight iliotibial band, hip flexors, quadriceps and hamstrings to improve mobility. Then strengthen phasic (weaker) hip abductors (glute medius and minimus).
Strengthening specifically hip abductors in various studies, when compared to general strengthening resulted in significant reduction in knee pain, objective change in functional outcome tests, physical function and daily activities(Bennell,K.L., et al. 2010 & Hernández-Molina, G. et al. 2008). Core strengthening should also be an integral part of the training program and personalized.
Exercises to avoid: Single leg and deep squats (places excessive compression forces on hip joint).
The determination to undergo a total hip replacement is primarily based and decided by both the surgeon and patient. Whereby a patient has significant inability to perform daily functional activities, experiences severe pain and lacks functional mobility.
Total hip replacement surgery
Hip replacement (THR)
In traditional hip replacement surgery, the surgeon makes a long incision and cuts various muscles, tendons and ligaments to get to the hip joint. When more tissues, muscles and tendons are cut during surgery, the recovery is more painful and the healing process takes longer.
Hip replacement surgery has evolved into one of the most frequently performed reconstructive procedures today. In the total hip replacement surgery, the surgeon can perform either a posterior (back), lateral or anterior (front) approach.
Recommendations for training: Important to follow hip precautions: avoidance of crossing affected leg towards midline (adduction) and squatting past hip flexion 90 degrees.
Training should focus on strengthening weak glute medius and minimus, glute maximus and hamstring muscles.
Effective and safe exercises include: in place lunges, diagonal lunges, seated leg extension and seated leg curl machine.
Core strengthening should also always begin with static exercises and then progressed to dynamic accordingly. Safe and effective core strengthening exercises include standing trunk rotation with tubing or cable, four-point planks and side planks. Safe dynamic core strengthening exercises include bridging with physioball, single leg bridge with physioball, traveling forward lunge with medicine ball trunk rotation and four-point plank on physioball as examples.
Contraindications to training: Patient should avoid deep squatting and single leg squats, which can compromise the prosthesis, making it susceptible for dislocation and creating deep hip pain.
The hip is a complex unit that is comprised of a multitude of ligaments, tendons, connective tissue and muscles that synergistically initiate and correct movement and stabilize in an unstable environment. Understanding the anatomy, biomechanics and weak links of the hip, common injuries and evidenced-based training strategies, should provide you with the insight to better understand and work with clients with these kind of injuries more confidently.
REFERENCES
Bennell, K.L., et al., 2010, 'Hip strengthening reduces symptoms but not knee load in people with medial knee osteoarthritis and varus malalignment: a randomized controlled trial,' Journal of Osteoarthritis and Cartilage, vol. 18, issue 5, pp. 621-628.
Cyriax, J. 1982, Textbook of Orthopedic Medicine, Volume 1: Diagnosis of Soft Tissue Lesions. London, UK. Baillere Tindall.
Fernandes, L., et al 2010, 'Efficacy of patient education and supervised exercise vs. patient education alone in patients with hip osteoarthritis: a single blind randomized clinical trial,' Osteoarthritis and Cartilage, vol. 18, issue 10, pp. 1237–1243.
Hernández-Molina, G., et al., 2008, 'Effect of therapeutic exercise for hip osteoarthritis pain: Results of a meta-analysis,' Journal of Arthritis Care & Research, vol. 59, issue 9, pp. 1221–1228.
Hinman, Rana S., et al 2007, 'Aquatic Physical Therapy for Hip and Knee Osteoarthritis: Results of a Single-Blind Randomized Controlled Trial,' Journal of Physical Therapy, vol. 87, no. 1, pp. 32-43.
Khayambashi, H., et al., 2012, 'The Effects of Isolated Hip Abductor and External Rotator Muscle Strengthening on Pain, Health Status, and Hip Strength in Females With Patellofemoral Pain: A Randomized Controlled Trial,' Journal of Orthopedic Physical Therapy, vol. 42, no. 1, pp. 22-29.
Lankhorst, N, et al, 2012, 'Risk Factors for Patellofemoral Syndrome: A Systematic Review,' JOSPT, vol. 42, No. 2, pp. 81-90.
Meira, E., et al., 2011, 'Influence of the Hip on Patients With Patellofemoral Pain Syndrome,' Sports Health, vol. 3, issue 5, pp. 455–465.
Pisters, M., et al., 2007, 'Exercise adherence improving long-term patient outcome in patients with osteoarthritis of the hip and/or knee,' Arthritis Care & Research, vol. 62, issue 8, pp. 1087-1094.
Prock, S., 2007, 'Initial results with a mini-posterior approach for total hip arthroplasty,' International Orthopedics, vol. 31, supplemental 1, pp. 17–20.
Sutlive, T., et al, 2008, 'Development of a Clinical Prediction Rule for Diagnosing Hip Osteoarthritis in Individuals With Unilateral Hip Pain,' JOSPT, vol. 38, no. 9, pp. 542-548.
Zhang, W., et al., 2007, 'OARSI recommendations for the management of hip and knee osteoarthritis, Part I: Critical appraisal of existing treatment guidelines and systematic review of current research evidence,' Osteoarthritis and Cartilage, vol. 15, issue 9 pp. 981–1000.